
Routine immunisation alone is not enough. Even where services exist, children are still consistently missed.
In a remote village in the Democratic Republic of the Congo (DRC), I recently slept in a health centre 200 km from any urban hub. My goal was to see what was really happening on the ground. The facility was stocked, the vaccines were cold, and staff were present. On paper, routine immunisation was functioning.
Yet, one child I saw at the facility – 23 months old and eligible for multiple vaccines – had never received a single dose. He wasn’t hidden in an unreachable village many kilometres away; he was standing right inside the clinic.
The reason he was still a “zero-dose” child? The staff didn’t want to “waste” a multi-dose vial on just one child. Because he had arrived alone, the cost-efficiency of the vial was prioritised over the life of a single child. He had shown up at the “wrong” time, and no one had told his family when the “right” time was.
The need for change
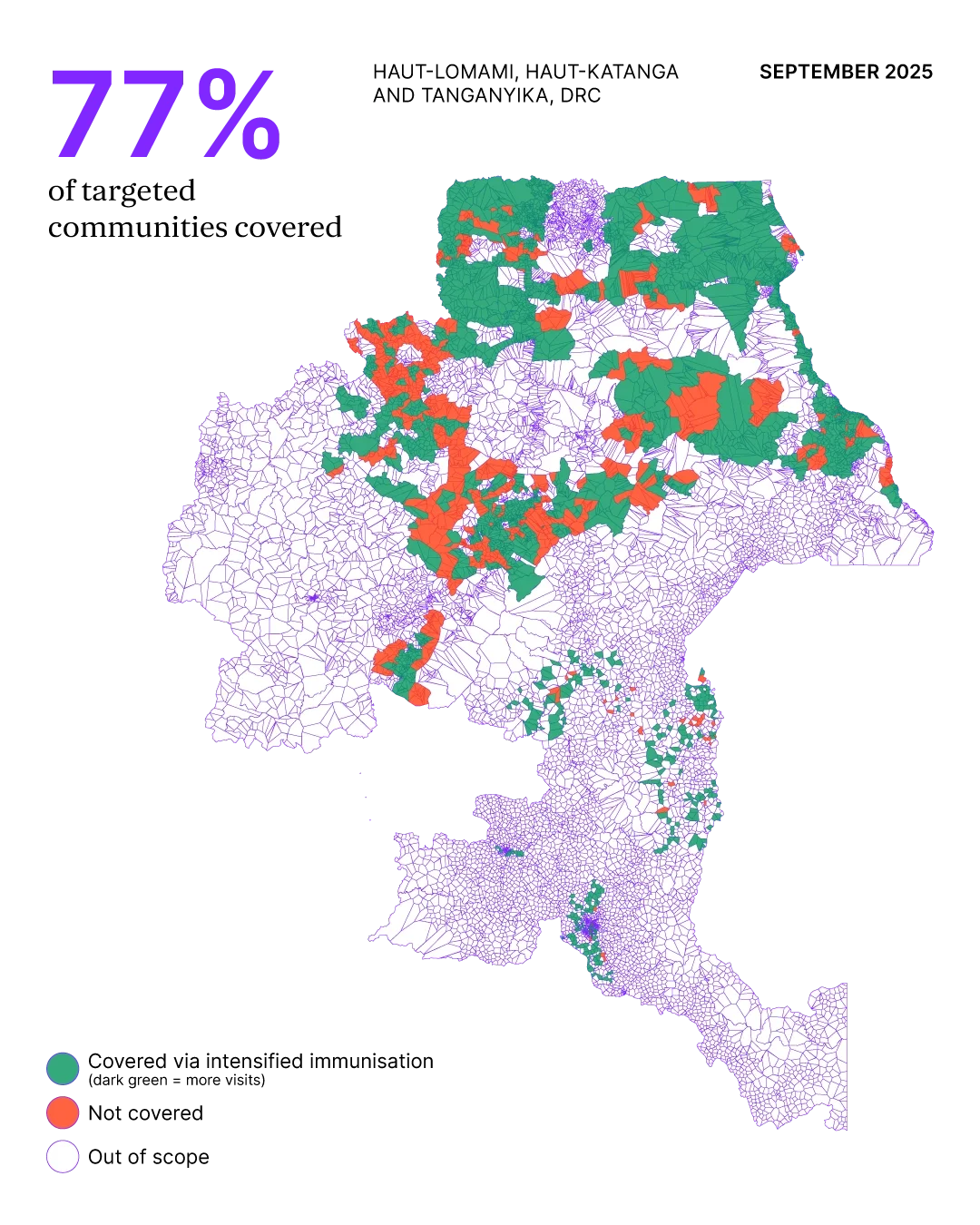
Simply launching more “intensified” immunisation rounds wasn’t the answer. Provinces in the DRC already conducted intensified vaccination rounds three times a year. They were intended to boost coverage, but the issue was execution.
Teams were identifying missed children only after rounds had already ended. Dates were not communicated. Vaccination hours were designed for the convenience of the clinic, not the schedule of a working mother.
The consequences were visible in the data. Between 2022 and 2024, full immunisation coverage in Haut-Lomami province – home to 4.5 million people – plummeted from 90% to 50%. Outbreaks inevitably followed. Measles cases arose because the system was blind to the children standing right in front of it.
Seven days, used differently
To fix this, we turned the seven-day intensification model on its head. Instead of waiting passively at facilities, teams moved into the community before the first vial was even opened.
-
Precision mapping: We moved away from vague estimates and shifted toward “polygons”. This is digital mapping that identifies specific clusters of households. It allowed us to prioritise 170 high-risk areas, rather than thinning out resources across entire provinces.
-
Tailored mobilisation: Existing demand data showed that around 50% of missed vaccinations were due to a simple lack of awareness. We mapped and engaged the trusted voices of influential community members, including village elders, religious leaders, and community health workers, to ensure every family knew exactly when and where to be. In urban areas, where technology was more widely accessible, other communication channels like radio were used in combination with community influencers.
-
Real-time feedback: The government deployed supervisors to check demand generation in real time. If turnout was low on Tuesday, we didn’t wait until the following month to react. We adjusted the messaging or moved the vaccination site by Wednesday.
Mohamed Taktak, Project Manager for Acasus in the DRC, coaching District Health Managers on microplanning for measles vaccination in Kamina, Haut-Lomami Province.

Adapting to local realities
The clearest lesson from the field was that service delivery must fit daily life, not the other way around. In many villages, mothers were in the field from dawn until dusk. By shifting vaccination sessions to start at 5 am or 4 pm, the service became accessible.
In conflict-affected areas like Tanganyika, the challenge was even steeper. Here, our team worked with local organisations experienced in humanitarian dialogue. These intermediaries, who are often respected local figures who maintain strict neutrality, negotiated directly with armed group leaders.
These intermediaries leaned into a pragmatic reality. It is often in the interest of rebel groups to allow vaccination. It shows the local population that they can provide, and it shows the government they can govern effectively. By using intermediaries who did not side with the government or the rebels, we secured safe windows for vaccinators to enter “red zones”. These negotiations were the difference between a protected child and an outbreak.
What changed
After three periods of routine intensification adapted to meet local needs, over 72,000 children aged 0–59 months were fully vaccinated against measles. Over 95% of communities received full measles protection across Haut-Lomami, Haut-Katanga and Tanganyika – three of the country’s southeastern provinces, where the disease was most prominent.
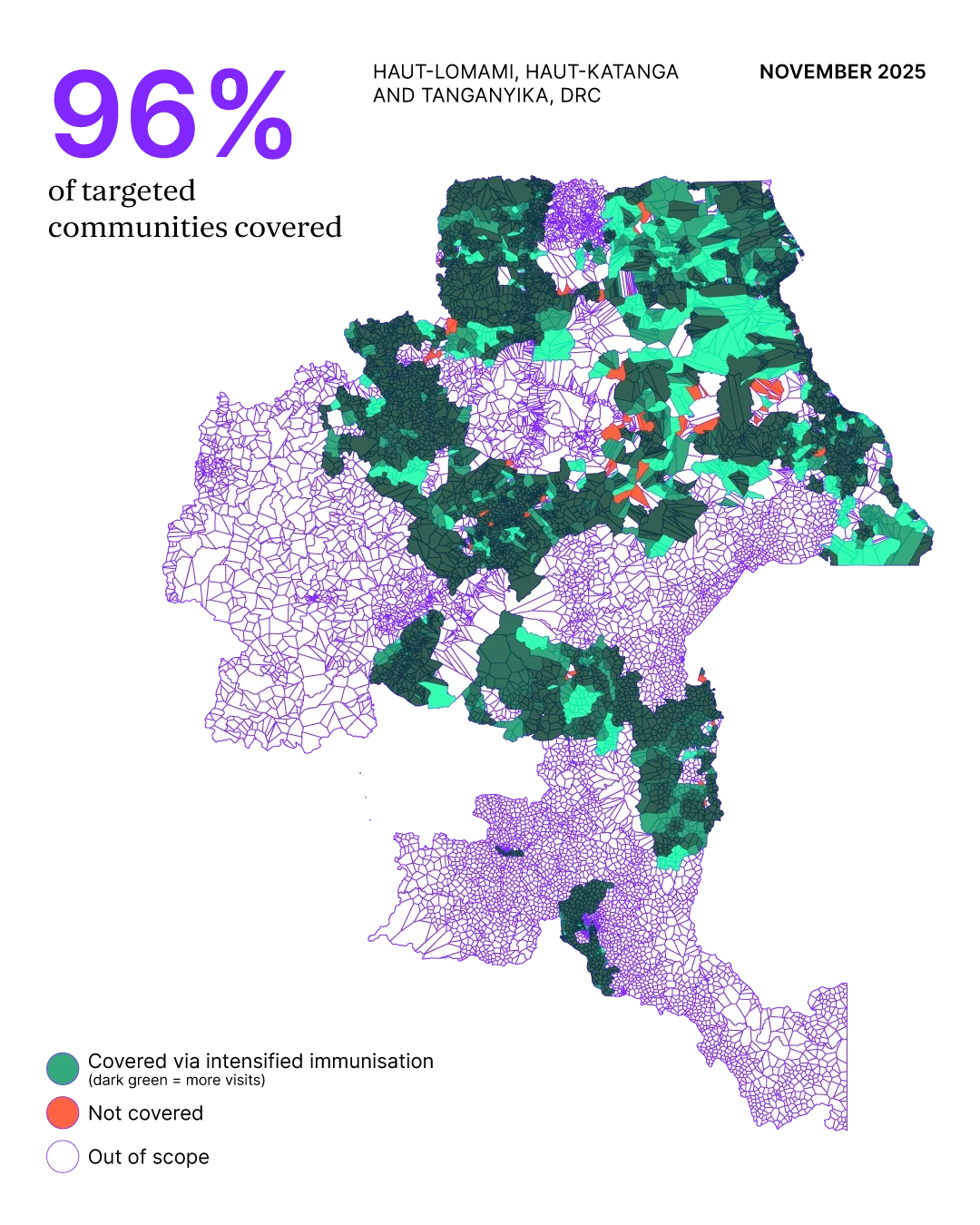
Equally important is that provincial teams developed better habits: tailored demand, stronger coordination, and a sharper focus on follow-through, which will enable long-term sustainability.
This work was led in close collaboration with Arthur-Nils Dufayard, Senior Project Manager for Acasus in the DRC. To learn more about how we help governments improve healthcare, read about how we supported Nigeria to reach children living with HIV.

