
Good nutrition is the foundation of public health. A well-nourished child fights off deadly infections better, and mothers have a safer chance of surviving childbirth. So why is nutrition often treated like the forgotten ‘orphan’ of public health?
In April 2025, health leaders in Tete Province, Mozambique, faced a watershed moment. Data showed that 66% of remote villages were being completely missed by health workers. While sudden foreign aid cuts contributed to the strain, there were deeper problems: a fragmented infrastructure where separate health teams (from nutrition, to malaria and HIV) operated in strict isolation. With individual budgets stretched thin, the nutrition team originally had only enough resources to reach two districts, leaving the rest of the province’s children with nothing.
Moving Beyond Siloes
The rainy season amplified the isolation of separate teams. Dirt roads turned into thick mud, stretching short trips into days-long journeys. For a mother living in a remote village, seeking care meant enduring a gruelling 20km walk to a clinic. If she braved the walk to get her child a routine vaccine, she would need to make the same journey weeks later just to get a malaria net.
Health leaders in Tete realised they could no longer afford to run separate, isolated programs. The solution was not a new, expensive tool. It was to bring different teams out of their separate boxes to pool their fuel, vehicles, and staff.
Instead of separate teams driving multiple cars down the same muddy roads, the nutrition team began ‘piggybacking’ on the immunisation programme, which still had resources. By launching integrated mobile brigades, a single vehicle now carries a multi-disciplinary health team. In one community visit, a mother can access a full package of care simultaneously: her child is screened for malnutrition, completes routine immunisations, and receives a malaria net.
An integrated outreach team in Tete Province, sharing a vehicle on its way to deliver immunisation, nutrition, malaria, and HIV services to remote communities.

This small shift allowed different partners and managers to sit at the same table and manage resources together. Weekly data dashboards from the health facilities gave managers clear visibility on stock levels, helping them quickly ship out supplements before a remote clinic ran completely dry.
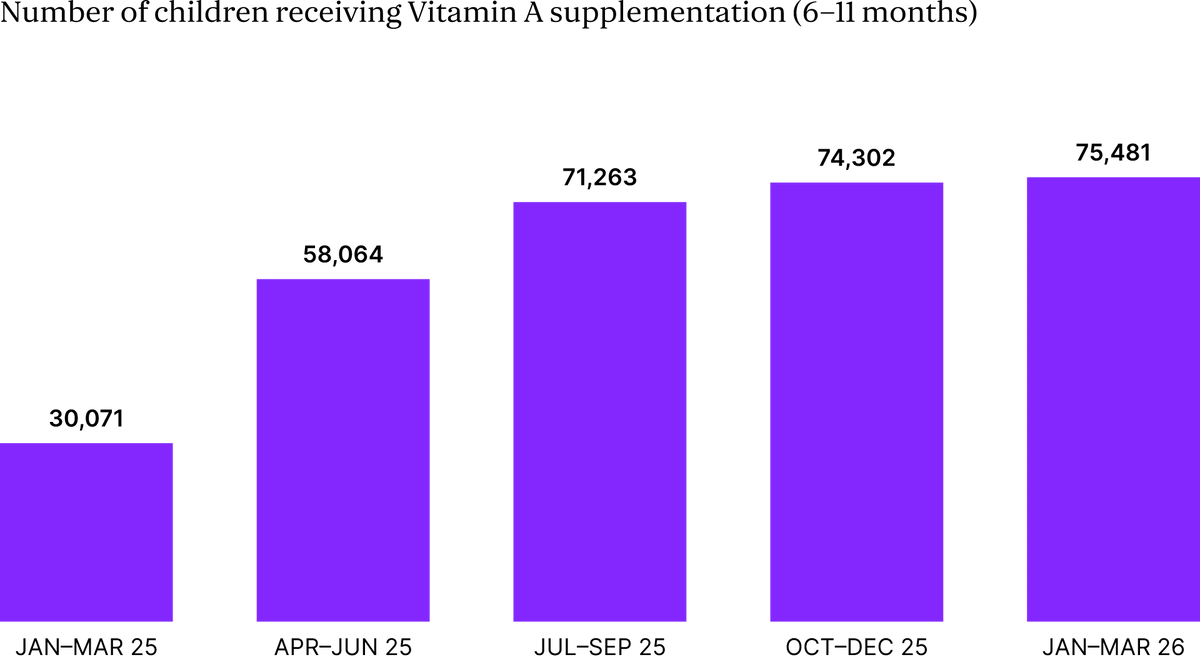
The long-term data proved that sharing resources worked. Within a year of moving to this new way of working across seven provinces, the number of children aged 6 to 59 months receiving vital Vitamin A supplements more than doubled, jumping from 90,212 to 182,282. In the same period, deworming treatments for children aged 12 to 59 months increased from 64,274 to 105,806.
The results were so strong that the Minister of Health recommended every province to adopt this model. By packing nutrition and basic care into the same vehicle, Mozambique is proving that simple coordination turns a hidden problem into a life-saving solution.

